
CUSTOM FOOT ORTHOTICS, ORTHOPAEDIC BRACING, FOOTWEAR
Back2feet Inc.
(416) 335-3701
*By Appointment Only*
CUSTOM FOOT ORTHOTICS, ORTHOPAEDIC BRACING, FOOTWEAR
716 Gordon Baker Road
Suite 700 (Ground Floor)
Toronto (North York), Ontario, M2H 3B4
Bracing in CMT
One of the more challenging disorders affecting the neuromuscular make-up of the foot is Charcot-Marie-Tooth disease. In this disorder a degenerative process occurs without any swelling which affects the cells of the spinal cord which control the function of skeletal muscles and peripheral nerves.
The clinical picture frequently seen is peroneal muscle and tibialis anterior weakness (the muscles that allow you to lift your foot), and decreased tone resulting in a floppy drop foot which has the tendency to turn down and in and is difficult to control. The CMT person has to compensate their walking by lifting and bending the knee excessively to prevent the toe from dragging during the swing phase. This is known as steppage gait. The CMT person also has problems with the leg collapsing forward over the foot resulting in the knee giving out. This steppage gait is compensated for by allowing the knee to extend to the back beyond its normal range during the stance phase to keep the weight in front of the knee preventing premature unlocking of the knee to avoid falling.
The unopposed muscles, the tibialis posterior (which supports the arch) and long flexors of the toes causes the exaggeration of the longitudinal arch as well as a tendency for the foot to turn in. This leads to a foot that weight bears on the outer border frequently pressing and/or moving against the side of the shoe. This results in shearing stresses from movement of the foot within the shoe which adds pressure on bony prominences with an increasing tendency for callousing and/or skin breakdown.
Quite often the CMT person will experience the decrease in the ability to feel in the affected areas, and if not careful, this may lead to blisters, sores, breakdown and even infection of the skin. This decrease in sensation also affects the CMT person in their ability to maintain balance, compromising the body's ability to make proprioceptive adjustments (knowing instinctively where your body is in space). Along with muscle imbalances and resulting lax or overstretched ligaments and altered weight bearing surfaces, there is the increased tendency to sprain or twist ankles. Often this vicious cycle results in wear and tear of joints and eventually leads to pain.
With state of the art plastics, foams and materials, and newly developed techniques used by orthotists in the last 15 years, orthotists who have faced the varying problems of atrophying disorders have certainly been tested in being able to create some truly interesting and workable new orthotics.
Orthotic Management
Orthotic management of the lower extremities for those with CMT can be grouped into three categories:
Group One: Those who require medial-lateral (side to side) stability and weight distribution to their feet can be fitted with foot orthotics.
Group Two: Those who require medial-lateral (side to side) stability, weight distribution and drop foot control, depending on severity, can be fitted with a wide variety of off-the-shelf ankle splints to customized ankle/foot orthoses (AFOs).
Group Three: Those who require medial-lateral (side to side stability, weight distribution, drop foot control, accommodation and control of foot deformities can be fitted with customized tubular ankle/foot orthoses. Tubular AFOs differ from the ordinary ones in that they wrap around the entire foot and ankle.

FRONT VIEW: Note the heels are turned inward toward the midline of the body. The outside ankles are also very prominent because of the alignment of the foot.
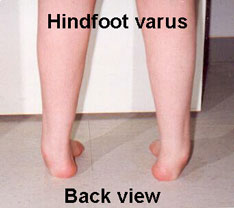
BACK VIEW: Note weight bearing is on the outer border of feet with the inner border of the feet raised and the toes are swinging towards the midline of the body.
Case Study: Catherine
Catherine is a very energetic female, mid twenties, diagnosed in her early
teens with CMT. Her paternal side showed signs of CMT but was never diagnosed
officially. She had a history of bilateral patella-femoral pain (both
kneecaps and thighs) which was eventually resolved when the cartilage
and patellae (kneecaps) were surgically removed. Over two and a half years
ago, she was having problems with twisted and sprained ankles and mild
drop feet. Tendon transfer procedures resulted in a better walking pattern
for approximately eight months. At this time, Catherine delivered her
third child and at which point, again, she began to have problems with
ankle instability, tripping and balance.
Catherine was assessed and fitted with custom plastic ankle/foot orthoses on both feet. These helped to improve her balance and walking pattern. Within a year, however, she began to experience a decrease in her sensation to her feet, claiming they felt cold all the time. In addition, she began to develop callousing over bony areas such as the ankle bone and the small prominence located on the outside of the foot. She also began to develop tightening in her achilles tendons (heel cords) and a high instep causing her foot to no longer fit the customized shaping of her AFOs. Her walking was also less stable from front to back and from side to side.
Catherine was reassessed as now having severe equinocavovarus (see definition at end) deformities. It was determined that these deformities developed as a result of increased deterioration of the muscles in addition to developing compensatory patterns for stabilizing the foot such as throwing her knees backward to shift body weight. An option open to Catherine was surgery to stabilize her foot which she adamantly declined. After much discussion and consideration, she was fitted with tubular ankle foot orthoses on both feet . These were designed to accommodate the foot and the bony prominences, we well as correct the various foot deformities.





View of tubular ankle/foot orthoses: Orthoses are held on by 2 velcro straps located at the top of the brace and at a 45 degree angle to the ankle. Trimlines of the orthosis are designed for ease of donning and doffing and for control of the foot. Orthosis can easily be opened to slide foot in. Note alignment of orthosis within the athletic shoe. There is still mild hyperextension at the knee so as not to compromise the compensatory mechanism.
The tubular AFOs have a lining of foam and leather where they touch the skin molded directly over modified positive casts of Catherine's legs. This allowed for cushioning and protection of the bony areas and support to her floppy feet. In addition, the lining provided added warmth as it acted as an insulator and wicked perspiration away from the skin. Within the padding was a build-up for the accommodation of the position of the foot equinus (position of deformity in which the foot is pointing downwards). The built-in equinus also helped to stabilize the knee, in effect assisting the compensatory mechanism developed. The plastic used was very thin, approximately 2mm thick, in some areas as thin as 1mm, flexible enough for Catherine's CMT affected hands to open, yet strong enough when in its tubular form to control and support her body weight. These tubular AFOs tended to be a bit bulkier than the standard plastic AFOs because of the foam and leather interface and circumferential design but were approximately of the same weight if not lighter.
I have worked with Catherine on her bracing needs for the past two years. During this time, we have developed a strong working relationship built on trust. I feel it is important as an orthotist to listen to your client and understand their problems and find a way to incorporate solutions into the orthotic design while not taking away any of the compensating mechanisms they have developed in order to be able to walk.
I would like thank Catherine for all her patience and cooperation as this was a challenging yet rewarding learning experience for me.
Definition of Equinocavovarus
Deformity of the foot in which the heel is turned inward toward the midline
of the body and the foot is pointing downwards.
This is associated with the raising of the inner border of the foot (supination/varus)
and displacement of the front part of the foot so that it lies towards
the body midline with respect to the centre of the leg (adduction).
With this foot, the arch is higher (cavus) and the foot is in equinus
(position of deformity in which the foot is pointing downward).
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()