
CUSTOM FOOT ORTHOTICS, ORTHOPAEDIC BRACING, FOOTWEAR
Back2feet Inc.
(416) 335-3701
*By Appointment Only*
CUSTOM FOOT ORTHOTICS, ORTHOPAEDIC BRACING, FOOTWEAR
716 Gordon Baker Road
Suite 700 (Ground Floor)
Toronto (North York), Ontario, M2H 3B4
Treating heel pain effectively with foot orthotics
Foot, ankle, lower leg or even knee pain is among the common problems that foot specialists see. Most cases are a result of biomechanical foot abnormalities such as the arches falling or, as in the case of CMT, the arches are increasing. In both situations, the heel position will be affected by the height of the arch when the person applies weight to the foot.
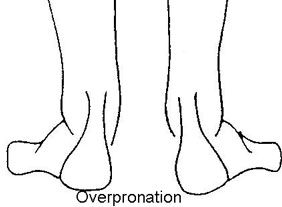
Low/Dropping Arches: While sitting the foot appears to have good arches, but when the person stands up, the feet clearly show flattening of the arches. This is accompanied with the ankles and the knees rolling in towards the body midline. Viewed from behind, the heel is seen to be turning outward as though the foot is displacing from under the ankle. This is accompanied with the front part of the foot swinging outward with most of the weight placed through the second and great toes This is known as overpronation of the feet causing the feet to be too flexible. When standing or walking in this situation the person may feel heel pain, arch fatigue and generalized pain in the lower legs. This results in an overuse syndrome where muscles and tendons have to work extra hard to compensate for the poor alignment of the foot. Often callousing is present over areas of great mechanical stress such as under the ball and the inner border of the foot.
FACTORS resulting in overpronation
- type and condition of footwear worn (dress shoes, safety shoes/boots
etc.)
- occupation (standing or sitting for long periods)
- body posture, weight gain
- presence of tight calf muscles
- ligamentous and muscle laxity
- bony alignment
- recent injury or trauma
- change/increase in activity
- health history
- age
One of the most common symptoms that people experience with overpronation is heel pain. The heel pain may be located around the outside of the heel or be at the centre of the heel bone or it may be located along the inner edge of the heel. Often pain will also be felt along the length of the arch. More often than not, this heel pain is also associated with general achiness about the outside ankle and shin splints (pain located on the front of the leg), sometimes pain may even radiate up the back of the leg.
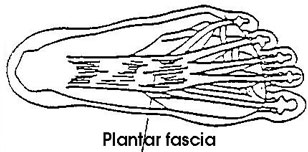
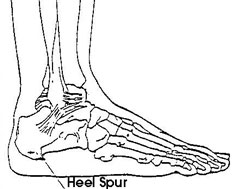
Over a period of time the long, supportive band of tissue (plantar fascia) that runs along the bottom of your foot from the heel, through the arch and into the ball of your foot becomes strained. Because the plantar fascia does not have much ability to stretch it suffers microtears with the continual stain. These small tears heal with scar tissue. Scar tissue has even less ability to stretch than the original tissue so any further strain results in inflammation. This becomes an unpleasant vicious cycle. This condition is called plantar fascitis. The pain from plantar fascitis is most severe when you first get out of bed and put weight on your foot. The pain decreases as you get going but reoccurs and may get worse throughout the day and after periods of rest. The chronic stresses to the plantar fascia may also cause a heel spur to develop; this is the body's way to try to strengthen the heel bone where the plantar fascia is attached. The heel spur itself is not painful. It is the microtears and subsequent inflammation that causes the pain.
As with so many other foot problems, conservative treatment, such as
rest, ice, anti-inflammatory drugs, taping, heel pads, exercises and physical
therapy will help but the problem will often recur if poor foot mechanics
go uncorrected. Foot orthotics which correct deforming forces and
provide good support can be used together with the above to provide relief.
These devices ae worn inside of supportive footwear for all weight-bearing
activities.
High/Increasing Arches: In people with high arches, in about two thirds of these cases there is an underlying neuromuscular disorder; of these, one half is CMT. These feet tend to underpronate and are variable in degrees of rigidity. The rest of this article will focus on the CMT foot.
CMT is an inherited degenerative disorder resulting in progressive foot
deformities. Symptoms are primarily motor, typically affect the lower
limbs, but hand and forearm involvement may also be present. Neuropathic
wasting creates imbalances between pairs of muscles which results in deformities.
Due to the relatively consistent sequence of selective muscle wasting
a characteristic foot type can be observed.
The usual order of wasting and deformity seen:
Wasting:
- small muscles of the front part of the foot (foot intrinsics)
- muscle on the outside of the leg (peroneus brevis)
- muscle on the front of the leg (tibialis anterior)
Deformity:
- claw toe deformities
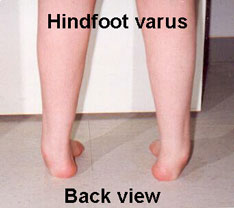
- forefoot adduction and hindfoot varus, where the forefoot and the heel
of the foot is swinging toward the body midline. The foot assumes a "C"
shape appearance
- dropped great toe, forefoot valgus, drop foot
With these combinations of foot deformities, the front part of the foot is twisted with the great toe tilted lower than the fifth toe. To get the foot to be flat on the ground at the time full weight is applied to the foot, the heel must roll in towards midline of the body. This results in an unstable foot as the body weight goes through the outside of the ankle which is now prone to frequent turning.

CMT foot complaints (in earlier stages):
- deep heel pain from excessive tensile stress to the heel attachment
relating to the elevation of the arch
- foot fatigue due to foot and ankle weakness
- ankle instability aggravated by poor proprioception
- metatarsalgia and irritated claw toes
- increased callousing over pressure areas
- outer border foot pain secondary to overload
- poor tolerance of impact loading
Associated complaints (in later stages):
- poor balance
- side trunk bending resulting in a waddling appearance
- increased lifting and bending of the hip and knee to clear the floor
- low back pain due to increased curvature to lower spine
- knee hyperextension
- knee cap shifting/subluxation
- poor ankle control (foot slapping/toe dragging)
- calves with wasted appearance
- increasing degree of sensory loss
CMT orthotic management can be broken down into three overlapping groups depending on the severity:
Group one: Foot orthotics can be fit for those who require medial-lateral (side to side) stability and weight distribution to their foot. The foot is still flexible and will respond well to conservative treatment. This is for those who can walk well with minor foot problems but find they tire very easily and their balance is progressively getting poor. Various foot deformities onset may be delayed by a foot orthotic providing good motion control, weight distribution and support. Supportive footwear will also assist in balance and control.
Group two: In this group, medial-lateral stability, weight
distribution and mild dropfoot control is required. The foot flexibility
is decreasing but the foot can be positioned. Foot orthotics with supportive
footwear and shoe modification provides much support in moderate ambulation
but for longer distances and when the person tires ankle control is required.
In some cases, a variety of off-shelf ankle splints/braces may provide
some support in conjunction with the foot orthotics.
(Please note:
these are generally used as an assessment tool and not to be worn long
term.) Customized ankle foot orthoses (AFO) with a varying degree
of support may be indicated depending on severity.
Group three: In this group the condition is severe, the foot requires medial-lateral stability, weight distribution, dropfoot control, accommodation and control of foot deformities. Customized bracing with various shoe modifications is indicated for this group. Conservative treatment becomes difficult when the deformities progress to extreme rigidity leaving surgery to be the only alternative.
Abnormal foot biomechanics with recurrent symptoms should be thoroughly
examined and assessed by your physician, who can then refer you to a foot
specialist for an orthotic device. Properly designed, an orthotic controls
the mechanics of the foot through all phases of gait, from heel contact,
to foot flat, to toe off. While the evaluation is important for the proper
device, the follow-up of the orthotic is vital for the success of the
device. The foot specialist must determine how well the orthotic is correcting
the abnormal biomechanics. Progress of the individual should be monitored,
as adjustments will be required; it is not uncommon to have two to three
follow-up visits.
Prescribed orthotics used as a complement with other modalities such
as rest, exercise, anti-inflammatory drugs, and in some extreme cases
surgery, can provide much relief to those who have foot and leg pain.
The importance of appropriate footwear and orthotic devices cannot be
overemphasized for the CMT population. Increased function and the level
of comfort provided by conservative care prevents injuries and may even
postpone the need for surgery.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()